Posted 11 September 2013
Susan’s Battle Against Migraine
Another campaign launched in 2012
Susan decided last year to try again to find an effective treatment for her migraine headaches. During 2011 and 2012 the headaches were generally pretty bad — even more frequent and painful than they had been before.
She was referred to a doctor in Fort Smith, who spotted a possible problem in her cervical vertebrae and sent her to a neurosurgeon. He recommended surgery to remove some bone growths which were pressing on her spinal cord. The problem is not rare. It is called stenosis.
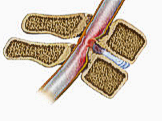
The growths were not declared to be causing, or even contributing to, the headaches, but they needed to be removed lest they begin affecting nerve function.
After the successful surgery to remove the bone growths last fall there was no noticeable difference in the headaches, and Susan was referred to another Fort Smith neurologist with expertise in migraines, Dr. Jon Gustafson.
In December of 2012, Dr. Gustafson began a treatment program using two drugs:
(1) an anti-seizure agent called topiramate, which is intended to prevent constriction of blood vessels in the brain, and
(2) an anti-depressant called amitriptyline.
He started Susan on 50mg of each drug daily, then on succeeding monthly visits increased the daily dosages to 100mg, then 150mg, then to 200mg in May. There were some strong side effects with all dosage increases, but each time the effects dissipated within a few days until Susan reached the 200mg-a-day level.
The side effects have not dissipated at this level.
In addition to the two drugs prescribed by Dr. Gustafson, Susan also uses venlafaxine, an anti-depressant she has been prescribed for several years since a now-abandoned migraine treatment program with another physician. Many of the negative effects Susan is experiencing were associated with this drug in manufacturer trials.
We have speculated that perhaps the daily dose of a second anti-depressant has enhanced these troubling side effects. We intend to ask Dr. Gustafson if the venlafaxine dose (which he knows about but did not prescribe) is necessary or desirable.
Headaches not yet vanquished
Meanwhile, the headaches are still around, but Susan agrees they are (most of them) milder, not as frequent and not as enduring as before. Progress is being made, but it has been a long slog. Dr. Gustafson is not saying Susan someday soon will wake up and be headache-free. He is not even saying that she will become headache-free in 2014.
He is saying that she can look forward to someday being free of headaches most days of the month, maybe as many as 25-28 days out of 30. That is an appealing goal, given Susan’s past history, especially her 2012 experience of having bad headaches 8 or 9 days out of 10.
Right now the principal concern is the side effects of the drugs, which I would rate as nothing less than serious.
Drug side effects are relentless
Susan’s main problems are disorientation, inability to focus thoughts, occasional slurred speech, imprecise or incorrect language, inability to think of the word she wants (usually a noun or proper name), serious short- and medium-term memory deficiency, unsteady movements, nausea and problems with balance, muscle weakness and drowsiness.
Most of these symptoms were seen with prior dosages, but they are more pronounced and generally unrelenting at the 200mg dosage — especially the speech, the memory, the nausea and the unsteadiness.
The continuing side effects from her medications are especially worrisome to everyone who knows Susan well, because she has become a different person. She has been active for several years in certain community and social affairs, but the drugs have rendered her generally unable to participate in these activities.
For example, Susan was an active and expert quilter, even teaching classes on quilting techniques at several quilt guilds where she was a member. Now she cannot quilt. The complexity of it is beyond her, and she hasn’t touched her sewing machine for more than 10 months.
She was an organizer of events and a project leader in various venues. No longer.
Susan was an expert cook, able to construct excellent entrées from scratch without a recipe. That does not happen now. After losing some skirmishes with both kitchen range and microwave, she doesn’t have much confidence in the kitchen beyond the can opener and the cutting board.
Although there are times when Susan appears to be having a good day and feels she could drive, I am no longer comfortable allowing that. There is always a risk that the good day will suddenly turn bad.
Intensity of side effects unpredictable
Susan’s condition changes markedly from one day to the next, and even from morning to afternoon to evening. We cannot predict.
Sometimes she understands that unusual things are happening to her brain, and sometimes not. Occasionally, a few hours later or the next day, she will realize that she was off the rails. But she never fully understands when she went off or how far off she was — only that she was off somehow.
The drugs have crippled her memory. Sometimes, Susan cannot remember something she and I discussed a few minutes earlier — often a topic that was timely and fairly important to her. I can never assume that she will remember an incident, a conversation, an appointment or even what day it is.
Sometimes we will catch a rerun of one of our favorite TV shows and she will not recall that we watched the same episode as recently as two weeks ago.
Most distressing, her speech and memory symptoms mimic the kinds of disabilities manifested in persons with senile dementia or Alzheimer’s. That is particularly upsetting to me and the rest of our family and friends.
Susan is in a mellow mood almost all the time now. She never becomes angry or upset, even when a situation would seem to call for expressing irritation. Although I am pleased never to be a target of scolding or anger, the change of personality is worrisome.
Extended sleep is a common occurrence
Susan frequently is tired, and she probably averages 10-11 hours a day in bed. Sometimes she will sleep straight through 12 hours, or get into periods when she doesn’t fall asleep at a normal time and then will sleep from 3 a.m. to noon or 1 p.m.
Among the side effects of the drugs is dry mouth, which triggers a night-time cough, and this sometimes keeps her from sleeping soundly, which makes the tiredness worse.
Her sedentary life has weakened her physically. On August 26, on a rare trip out of the house, she lost her balance and fell in a Clarksville retail store, smashing her head and ribcage into a clothing rack. We spent the rest of the day at the hospital emergency room. Fortunately, scan and x-ray showed no breaks or internal damage. The doctor patched a 3cm cut on her forehead with adhesive.
After this incident, and an unsatisfying exchange of voicemails with the neurologist’s office, Susan agreed to my suggestion that she switch the venlafaxine dose to the afternoon instead of taking the entire chemical bomb at bedtime. So far, that change has been beneficial. She does not seem as detached and lethargic as before, and she seems much quicker to comprehend conversational topics — both in person and in television shows. She understands and responds appropriately to my ironies and sarcasms now, which had not been the case before switching the timing of the venlafaxine.
Susan’s headaches are less frequent and less debilitating than before she began this treatment. The improvement seems erratic: Some weeks she will have only a couple of mild headaches, other weeks she might have headaches three or four days, with one or two of them well beyond mild.
Overall, we are making some gains in this war on headaches. Victory still seems far off, but Susan is determined to see Dr. Gustafson’s program through.
About the drugs
Topiramate
This anti-seizure drug is often used in treating epilepsy, but it is also widely used to treat migraines due to the effect it has on the blood vessels in the brain. It is used as a preventative for atypical migraine sufferers. It widens blood vessels in the brain which have become constricted by increased serotonin levels. The two principal side effects appear to be memory deficiency and difficulty with speech patterns.
Amitriptyline
It is a tri-cyclic anti-depressant used for a number of medical conditions including: depressive disorders; anxiety disorders; attention deficit hyperactivity disorder (ADHD); migraine prophylaxis; eating disorders; bipolar disorder; post-herpetic neuralgia; insomnia; nocturnal enuresis (bedwetting) in children; cyclic vomiting syndrome; post-traumatic stress disorder (PTSD); chronic pain; tinnitus; chronic cough; carpal tunnel syndrome; fibromyalgia; vulvodynia; interstitial cystitis; male chronic pelvic pain syndrome; irritable bowel syndrome; diabetic peripheral neuropathy; neurological pain; laryngeal sensory neuropathy, chronic fatigue syndrome and painful paresthesias related to multiple sclerosis.